


Sponsored Article
Top Surgery & Male Chest Contouring: What's the Difference?
 When looking for a Top Surgery Surgeon, you may come across surgeons who make a distinction between Top Surgery and Male Chest Contouring. Understanding this subtle yet important detail is critical to achieving the Top Surgery results you seek.
When looking for a Top Surgery Surgeon, you may come across surgeons who make a distinction between Top Surgery and Male Chest Contouring. Understanding this subtle yet important detail is critical to achieving the Top Surgery results you seek.
By definition, the goal of Top Surgery is to create a masculine chest by "aesthetic contouring of the chest wall." The procedure is guided by four main principles:1
- Removal of breast tissue and skin excess;
- Proper reduction and position of the nipple and areola;
- Elimination of the inframammary fold;
- Minimizing chest wall scars.
Top Surgery is frequently described as a mastectomy with male chest reconstruction, which includes contouring the chest into a masculine shape.2 However, because of differences in patient anatomy and a lack of evidence based recommendations, there's no single best surgical approach to Top Surgery3, leaving its definition somewhat open to interpretation.
Some surgeons assert that Top Surgery alone doesn't achieve the "ideal male form"4 and that an additional cosmetic procedure called Male Chest Contouring, or simply Chest Contouring, is needed to realize this ideal.
Male Chest Contouring techniques include:
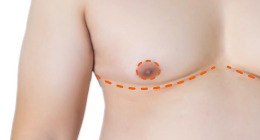
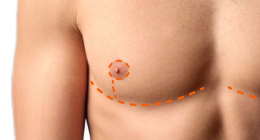
- Lengthened incisions to create a more masculine contour and reduce the risk of "Dog Ears";
- Liposuction to remove fat to enhance male contours;
- Internal sutures to reduce stress on the final closure sutures, to help minimize scarring and eliminate the need for drains.
Other surgeons consider these techniques to be integral to Top Surgery. For example, many surgeons favour using longer incisions to emphasize male chest contours and reduce the formation of Dog Ears (in Double Incision cases.)5,6 The elimination of contour irregularities is one of the most important aspects in all breast surgeries and many surgeons use liposuction for additional contouring, to help eliminate the inframammary fold, to avoid Dog Ears, and to attain better lateral symmetry.7,8,9,10 There's also a growing number of Top Surgery Surgeons who use an internal progression-tension suture technique by default to eliminate the need for drains. It's clear that asking your potential surgeons if they include any of these techniques—or if they charge extra for them—should be near the top of your list of consultation questions.
The root problem of why Male Chest Contouring isn't always included under the umbrella of Top Surgery is associated with the "aesthetic" component of Top Surgery and how it relates to medical billing.
"Aesthetic or cosmetic surgery is mostly regarded as not medically necessary and therefore is typically paid for entirely by the patient. In contrast, reconstructive procedures are considered medically necessary – with unquestionable therapeutic results – and thus paid for partially or entirely by national health systems or insurance companies. Unfortunately, in the field of plastic and reconstructive surgery (both in general and specifically for gender-related surgeries), there is no clear distinction between what is purely reconstructive and what is purely cosmetic. Most plastic surgery procedures actually are a mixture of both reconstructive and cosmetic components." — WPATH Standards of Care11
In Canada, Top Surgery is covered by provincial and territorial health plans, but Male Chest Contouring is viewed as cosmetic and may not be covered, leaving patients on the hook for costs ranging from $1000 to $2000 or more. Patients aren't required to have Male Chest Contouring but are advised that their Top Surgery results may not be satisfactory without it. The tissue that can cause Dog Ears is under the arms, often extending to the back, and not within the borders of the breasts, so its treatment isn't covered.
In the United States, some surgeons also charge extra fees for Male Chest Contouring techniques like liposuction because they're considered cosmetic by insurance companies and aren't covered.
 According to Top Surgery specialist Dr. Scott Mosser, singling out liposuction as a cosmetic procedure separate from Top Surgery doesn't make much sense. "Liposuction is just another tool that I can use when performing Top Surgery, " he says. In Dr. Mosser's practice, there are no contouring procedures beyond Top Surgery that are needed to reach a natural-looking endpoint.
According to Top Surgery specialist Dr. Scott Mosser, singling out liposuction as a cosmetic procedure separate from Top Surgery doesn't make much sense. "Liposuction is just another tool that I can use when performing Top Surgery, " he says. In Dr. Mosser's practice, there are no contouring procedures beyond Top Surgery that are needed to reach a natural-looking endpoint.
 Top Surgery expert Dr. Curtis Crane doesn't use liposuction when performing Top Surgery but does use lengthened incisions as well as internal sutures to eliminate the need for drains. His associates at Crane Center for Transgender Surgery, Dr. Ashley DeLeon and Dr. Gerhard Mundinger, also use these techniques, and there's no extra fee.
Top Surgery expert Dr. Curtis Crane doesn't use liposuction when performing Top Surgery but does use lengthened incisions as well as internal sutures to eliminate the need for drains. His associates at Crane Center for Transgender Surgery, Dr. Ashley DeLeon and Dr. Gerhard Mundinger, also use these techniques, and there's no extra fee.
 Using lengthened incisions and liposuction together to achieve great Top Surgery results has its roots in cosmetic breast surgery. Bra Roll Excision is a cosmetic breast surgery procedure that removes excess skin, fat or both that protrudes over, under and to the sides of bra straps. Dr. Hope Sherie, the popular Top Surgery surgeon in Charlotte NC, considers Bra Roll Excision a useful tool when performing Top Surgery.
Using lengthened incisions and liposuction together to achieve great Top Surgery results has its roots in cosmetic breast surgery. Bra Roll Excision is a cosmetic breast surgery procedure that removes excess skin, fat or both that protrudes over, under and to the sides of bra straps. Dr. Hope Sherie, the popular Top Surgery surgeon in Charlotte NC, considers Bra Roll Excision a useful tool when performing Top Surgery.
"If someone has excess skin on the sides of the chest which makes a crease or bra roll, then I extend the incision to remove that skin and flatten the sides of the chest. The incision can also be extended onto the sides of the back if needed," says Dr. Sherie. "If there is also a fat layer on the sides of the chest or a fat pad under the arms which will be thicker than the front of the chest after breast removal, then I treat those areas with liposuction."

26-year-old male, 2 years after Top Surgery - Buttonhole technique with Bra Roll Excision
Current best practices for the surgical approach to Top Surgery are mostly based on the personal preference and expertise of the surgeon12 so it's not surprising that methods differ. In your search for a Top Surgery Surgeon, be sure to ask about whether or not they include Male Chest Contouring in their definition of Top Surgery. Knowing where they stand on Male Chest Contouring will give you clarity about potential costs and a better chance of hitting your Top Surgery target.
What Do You Think?
References
1. Hage JJ, Bloem JJ. Chest wall contouring for female-tomale transsexuals: Amsterdam experience. Ann Plast Surg. 1995;34:59–66.
2. Male chest reconstruction, Wikipedia.com, https://en.wikipedia.org/wiki/Male_chest_reconstruction, accessed 04/10/20.
3. Ammari T, Sluiter EC, Gast K, Kuzon WM Jr. Female-to-Male Gender-Affirming Chest Reconstruction Surgery. Aesthet Surg J. 2019 Jan 17;39(2):150-163.
4. H. McLean, 'What Is Chest Contouring With FTM Surgery?', ftmtopsurgery.ca, 04/11/17, https://www.ftmtopsurgery.ca/blog/ftm-surgery/chest-contouring-ftm-surgery/, accessed 04/02/20.
5. Knox ADC, Ho AL, Leung L, Hynes S, Tashakkor AY, Park YS, Macadam SA, Bowman CC. A Review of 101 Consecutive Subcutaneous Mastectomies and Male Chest Contouring Using the Concentric Circular and Free Nipple Graft Techniques in Female-to-Male Transgender Patients. Plast Reconstr Surg. 2017 Jun;139(6):1260e-1272e.
6. Ammari T. et al.7. Monstrey S, Selvaggi G, Ceulemans P, Van Landuyt K, Bowman C, Blondeel P, Hamdi M, De Cuypere G (2008) Chest-wall contouring surgery in female-to-male transsexuals: a new algorithm. Plast Reconstr Surg 121(3):849–859
8. Lo Russo, G., Tanini, S., & Innocenti, M. (2017). Masculine Chest-Wall Contouring in FtM Transgender: a Personal Approach. Aesthetic Plastic Surgery, 41(2), 369–374. doi:10.1007/s00266-017-0796-0
9. Monstrey S. et al.
10. Bluebond-Langner R, Berli JU, Sabino J, Chopra K, Singh D, Fischer B. Top Surgery in Transgender Men: How Far Can You Push the Envelope? Plast Reconstr Surg. 2017 Apr;139(4):873e-882e.
11. E. Coleman, W. Bockting, M. Botzer, P. Cohen-Kettenis, G. DeCuypere, J. Feldman, L. Fraser, J. Green, G. Knudson, W. J. Meyer, S. Monstrey, R. K. Adler, G. R. Brown, A. H. Devor, R. Ehrbar, R. Ettner, E. Eyler, R. Garofalo, D. H. Karasic, A. I. Lev, G. Mayer, H. Meyer-Bahlburg, B. P. Hall, F. Pfaefflin, K. Rachlin, B. Robinson, L. S. Schechter, V. Tangpricha, M. van Trotsenburg, A. Vitale, S. Winter, S. Whittle, K. R. Wylie & K. Zucker Standards of Care for the Health of Transsexual, Transgender, and Gender-Nonconforming People, Version 7, International Journal of Transgenderism, 2012, 13:4, 58.
12. Ammari T. et al.